The kneecap surgery represents the final treatment for patients with recurrent knee cap dislocation. The process greatly reduces the chances of a recurrence of dislocation. It is especially indicated for young people and athletes.
Like any surgery, it is very important for the patient to collect as much information as possible about the surgical procedure to be taken, and to discuss its risks with the doctor or surgeon in charge. In this article, we will include all aspects related to the kneecap stabilisation surgery process and everything you need to know about this procedure.
An introduction to the kneecap stabilisation surgery
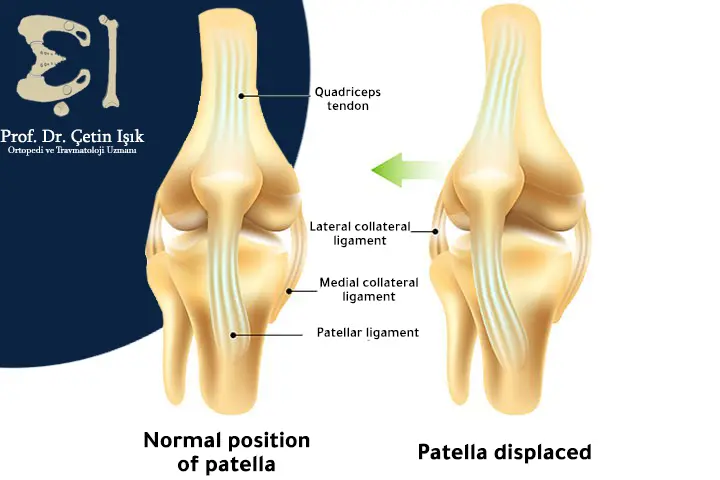
The kneecap or patella is a triangular bone located in the front of the knee joint. This bone can dislocate, so that the kneecap may deviate from its place.
Problems associated with the kneecap (patella) are common among practitioners of sports that require strong physical contact, such as soccer players, who commonly have either Kneecap fracture Or kneecap dislocation, there are two main types of removing the soap from its position, a traumatic type and a repeated type.
. kneecap dislocation can be treated either with conservative treatment (in most cases of traumatic dislocations) or with surgical intervention (in most cases of repeated dislocations).
When is the kneecap stabilisation surgery performed?
Doctors and specialists often prefer to perform kneecap fixation with conservative treatment and to give kneecap fixation exercises for prevention if this dislocation occurs for the first time, but in the event that the dislocation recurs, the kneecap fixation operation is carefully considered, the possibility of performing the operation depends on the following factors that play a decisive role in the surgeon's decision:
- Previous failed attempts to treat a dislocated kneecap with conservative methods increase the chances of surgical treatment being indicated.
- The extent of the damage to the kneecap bone and making sure that it is safe from fracture (the medical team performs the process of stabilizing the kneecap fracture in this case).
- In the event that there are risk factors or an incorrect placement of the ligaments or adjacent bones, surgery should be considered and conservative treatment should be discontinued.
- In the event that the patient is elderly or an athletic person, it may be indicated for him to perform joint surgery after discussing the advantages and risks of this procedure.
Types of kneecap stabilisation surgery
There are many surgeries that are performed to stabilize the joint, but the most important ones are:
Tibial tubercle transfer
The tibial tubercle is located below the patellar tendon. With this procedure, the tibial tubercle is moved up and to the center of the knee joint, and then fixed with screws. This fixation prevents the kneecap from slipping out of its original position. This type of operation is indicated for patients who have an external (lateral) position for both The tubercle of the tibial bone, in addition to the patellar ligament, which can be detected and confirmed by using a simple X-ray or magnetic resonance image, with which we accurately determine the location of the tibial tubercle in relation to the patella and femur.

lateral release
Arthroscopic procedure, a simple two-inch incision is made in the tight collateral ligaments that cause the kneecap to move out of place due to the tension of these ligaments on the cap, as this procedure supports the stability of the knee.

Reconstruction of the medial patellofemoral ligament (MPFL).
When the patella dislocates, the medial patellofemoral ligament is torn, which connects the lower end of the femur with the inner face of the kneecap, and the treatment is by implanting a new ligament or tendon that can be taken from any other part of the body, or from another body, plastic screws used to fix the patellofemoral ligament medially, and place it in the appropriate place that ensures good fixation of the kneecap.

Postoperative demonstrations of kneecap stabilisation surgery
The following signs and symptoms that may be seen normally after surgery include:
- Pain: The intensity of the pain of the kneecap fixation surgery decreases gradually with time, through the use of anti-inflammatory drugs and pain relievers. It is necessary to apply ice to the knee regularly (20 minutes every hour) during the few days after the surgery.
- Swelling and bruising around the leg or ankle.
- Knee stiffness: It is treated with physical rehabilitation exercises.
- Numbness and tingling around the knee joint, which diminishes with time, but a very small percentage of patients suffer from permanent numbness.
- Atrophy in the size of the quadriceps femoris muscle returns to its normal size by continuing the physical rehabilitation exercises.
Recovery after the kneecap stabilisation surgery
When you wake up after your patellar operation, your knee will be covered with a bandage. a physical rehabilitation specialist will come to you and give you instructions on the right methods to ensure your quickest recovery. You will need to use crutches for 3 to 5 days.
Physiotherapy aims to reduce swelling around the knee joint and to give exercises that protect the patient from any weakness or muscle stiffness. The physiotherapist sets specific appointments for you to see the speed of your recovery and make sure of the benefits of exercise.
A splint or brace is used for the first 6 to 12 weeks.
Risks and complications of kneecap stabilisation surgery
There are a number of risks related to surgery, including:
- Sepsis: 0.5 % is the probability of sepsis occurring after this surgery, it can be minor involving incisions made, or sepsis within the knee joint.
- Deep vein thrombosis (blood clots): 2% to 10% is the possibility of blood clots occurring in the veins of the patient's leg. It is rare for them to move to the lung and cause a pulmonary embolus. If you have leg pain after the patellar fixation operation, you must quickly tell the doctors. The case is managed by giving anticoagulants
- Recurrent dislocation: This occurs in 2% to 4% cases
- Fracture of the kneecap: There is a very small risk of a fracture of the kneecap during or after the operation.
- Permanent numbness and tingling may occur.
- Knee joint stiffness: In rare cases, it may require another surgical procedure. Physical therapy prevents recurrence.
- Weakness in the tendons of the knee joint.
- Continuous pain and swelling: It is common in the event of damage to the cartilage after the operation.
In conclusion, the process of fixing the knee cap reduces the possibility of a recurring dislocation of the knee cap. There are several techniques for this operation, each with its indications. Its benefits and risks are discussed with the surgeon, and follow-up is done with the physiotherapist.
Sources:
Common questions
The process of fixing the dislocation of the knee cap takes an average period of one hour to an hour and a half.
The knee cap moves normally when the leg is moved, but the knee cap moving out of its normal place is considered an abnormal condition.
Great blows and force on the knee joint lead to dislocation of the knee joint, and the connection between the femur and tibia is separated.
Symptoms of soap dislocation include severe knee pain and swelling, as well as difficulty bending the knee.

